Nipple pain occurs when repetitive high mechanical loads create epidermal or stromal inflammation

Nipple pain without visible damage is caused by excessively high intra-oral mechanical (or tensile) loads
The NDC nipple pain and damage clinical guidelines are developed from the emerging science of mechanobiology, which investigates the interaction between mechanical pressures and living cells, tissues and biological systems. You can find out about the science of mechanobiology here, and mechanobiology in breastfeeding here.
During suckling, the nipple epidermis, dermis and stromal core and other intra-oral breast tissue stretch in response to the mechanical force of vacuum. Vacuum is generated as the infant’s mandible drops in the context of a seal against the breast and the seal closing off the nasopharangeal space.1-3
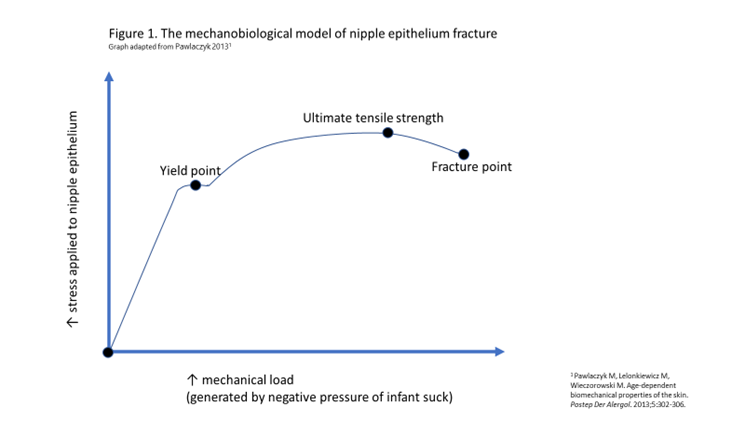
Elasticity of breast tissue and nipple-areolar complex skin varies widely between women. But epithelium begins to tighten at high stretch loads, known as the ‘yield point’, as the desmosome locking mechanism is triggered (see the figure below).4 5
The NDC mechanobiological model proposes two mechanical causes of nipple pain which result from suckling and also from mechanical milk removal.
Epidermal inflammation
-
Nipple pain results when stretching forces aren’t evenly distributed over a large surface area of nipple, areolar and breast skin, so that desmosomes in a focussed area of the nipple epithelium are subject to repetitive and excessively high mechanical loads or stretching forces.
-
This causes desmosomes to release cytokines and histamines, triggering inflammatory cascades in the absence of visible tissue damage.
-
If very high stretching or deformational forces are applied, a shearing load may also arise between the epidermis and dermis and the more stable interior collagen structure of the nipple, also causing release of cytokines and histamines and further inflammatory cascades.
-
Desmosome strain and inflammation in the nipple skin stimulate dermal nociceptors, triggering maternal nociception and perception of pain.
-
Stromal inflammation
-
Stromal microhaemorrhage results from vascular micro-trauma when the nipple is exposed to repetitive stretching, bending or deformational forces.
-
Microhaemorrhages trigger signalling pathways and an inflammatory cascade. Resultant increased stromal tension or swelling further perpetuates cascades of inflammatory responses.
-
The collagen-rich, highly vascular core of the nipple is threaded through with nerve bundles, which may also be vulnerable to mechanical stretching or deformational loads, and the effects of local inflammation.
-
Stromal microvascular haemorrhage and neural irritation trigger stromal inflammation, maternal nociception and perception of pain.
-
Persistent nipple pain
Persistent nipple pain results from persistent repetitive mechanical micro-trauma in the epithelium, dermis or stroma, which causes persistent inflammation. Inflammatory responses and associated nociceptor stimulation do not immediately cease with cessation of suckling or mechanical milk removal. But before the inflammation has had time to resolve, the nipple is again exposed to the mechanical load of milk removal.
The figure below illustrates the mechanobiological model of nipple epithelium yield (when tight junctions lock) and fracture (when the epidermis breaks). This graph adapted from Pawlaczyk 2013. 5
Why women may be particularly vulnerable to nipple pain and damage in the first week after birth
Women are particularly vulnerable to nipple pain and damage in the first week of breastfeeding. You can read about prevalence here.
-
This is because it takes time for the skin of the nipple to adapt and become more resilient in response to the mechanical loads of breastfeeding.
-
It's therefore important that women are educated in fit and hold strategies which distribute mechanical loads over as much nipple-areolar complex and breast skin as possible, to protect their nipples in the first days and weeks of breastfeeding.
Women often report that their nipples visibly change over the course of lactation. This also results from the way the nipple skin adapts to the repetitive mechanical loads of breastfeeding.
References
- Douglas PS, Geddes DB. Practice-based interpretation of ultrasound studies leads the way to less pharmaceutical and surgical intervention for breastfeeding babies and more effective clinical support. Midwifery 2018;58:145–55.
- Douglas PS, Keogh R. Gestalt breastfeeding: helping mothers and infants optimise positional stability and intra-oral breast tissue volume for effective, pain-free milk transfer. Journal of Human Lactation 2017;33(3):509–18.
- Douglas PS, Perrella SL, Geddes DT. A brief gestalt intervention changes ultrasound measures of tongue movement during breastfeeding: case series. BMC Pregnancy and Childbirth 2022;22(94):https://doi.org/10.1186/s12884-021-04363-7.
- Tepole AB, Gosain AK, Kuhl E. Stretching skin: the physiological limit and beyond. International Journal of Non Linear Mechanics 2012;47(8):938-49.
- Pawlaczyk M, Lelonkiewicz M, Wieczorowski M. Age-dependent biomechanical properties of the skin. Postep Der Alergol 2013;5:302-06.
- McClellan HI, Geddes DT, Kent JC, Garbin CP, Mitoulas LR, Hartmann PE. Infants of mothers with persistent nipple pain exert strong sucking vacuums. Acta Paediatrica. 2008;97(9):1205-1209.
