Galactocoele: investigation, management

Ultrasound investigation of suspected galactocoele
Differential diagnoses
On ultrasound a galactocele may appear similar to a
-
Lactating adenoma
-
Abscess
-
Fibroadenoma, or
-
Carcinoma.
However due to its pathophysiology, a galactocoele has no associated vascularity. Colour doppler interrogation shows no flow.
Ultrasound appearance
A suspected galactocoele may have a heterogenous and complex appearance ultrasonographically. This is due to
-
Its pathophysiology, discussed here.1 Milk composition includes water, protein, fats, and nutrients. The human body absorbs the components of milk at differing rates, resulting in radiological variation.
-
Its mixed structural composition. Of galactocoeles,
-
50% are cystic or multi-cystic
-
37% are mixed (solid and/or cystic)
-
13% are solid.
-
As a result, on ultrasound a galactocoele is
-
Anechoic and simple, or
-
Mainly anechoic with some diffuse echoes and multiloculated, or
-
Diffuse echogenicity ranging from moderate to highy echogenic.
On imaging, movement of the contents can be demonstrated by compression with the transducer. There are no blood vessels although flow may be demonstrated in the walls with colour dopper. Galactocoeles can appear with either a classic fat-fluid level or an indeterminate heterogenous complex mass.2,3
Triple assessment is typically required to confirm the diagnosis of galactocoele
Aspiration is often required for diagnosis. As a result, a suspected galactocele typically requires triple assessment to clarify the diagnosis:
-
Ultrasound
-
Aspiration 2
-
Histology.
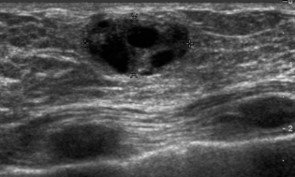
Images 1-3 below show the grossly varied appearances of galactocoele on ultrasound. All three of the following ultrasound images are lesions that were diagnosed as a galactocele after the aspiration.
Image 1
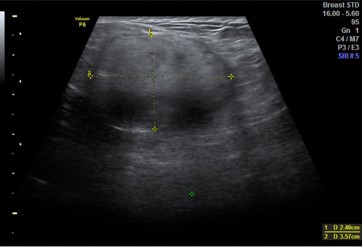
Image 2
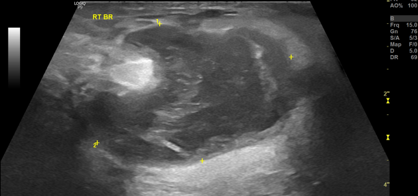
Image 3
Management of galactocoele
"If it ain't broke, don't fix it!"
A galactocoele requires no management.
-
Women are advised to leave the lump alone, and to not apply massage.
-
Some breast surgeons propose, from clinical experience, that a galactocele larger than three centimeters requires serial aspiration, or drainage and incision.
-
Drainage is also required if a galactocoele becomes inflamed or infected (or activates), in which case it has shifted on the spectrum of breast inflammation in lactation, to become an abscess.1, 3 You can find out about management of abscess here.
The pathophysiology of a galactocoele relates to decreased milk flow from the ducts (here) which leads to milk retention, and is not an infective process. All milk, including in a galactocoele, contains a microbiome. Since the galactocoele currently isn’t infected, there is no need to subject the patient to the risk (however small) associated with any kind of aspiration or incision. Time may allow for tissue remodelling and absorption of the galactocoele.
However, if the galactocoele is causing significant pain or develops signs of infection, it is now “broke” so it needs fixing!
What if a galactocoele becomes infected?
It is very rare for a galactocoele to become infected. This occurs most commonly after fine needle aspiration.
On the spectrum of breast inflammation, an infected galactocele has become an abscess, and is no longer a galactocoele. So now the question now is how to manage a lactational breast abscess. You can find out about this here.
What if the galactocoele is solid?
The solid galactocoele, or a galactocoele which has crystallised, is exceptionally rare and has had less than ten reports in the literature to date, with the majority of the reports from India.
The hypothesised pathophysiology of a solid galactocoele is that fat and proteins within the stagnant breast milk precipitate. This leads to the formation of crystals which are identifiable on testing after a fine needle aspiration. In this case, when fine needle aspiration is performed, the aspirate is typically a thick, chalky white material with a “gritty” sensation.
On histology, cytosmears show amorphous proteinaceous material along with crystals of varying sizes and shapes and are birefringent on polarising microscopy. Crystals demonstrate positivity for periodic acid Schiff and are weakly positive for calcium by the von Kossa technique. With H&E staining the images show with the presence of crystals in an amorphous, granular proteinaceous background and crystal polarisation.4,5
If the galactocele is heavily crystalised, almost becoming “solid”, it is very unlikely to spontaneously resolve. And in select cases given the extent of crystallisation the galactocele may require surgical excision.
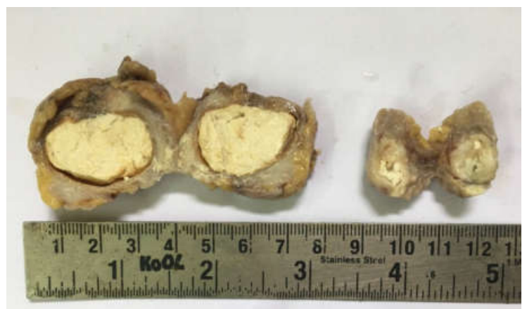
The images below are of a solid galactocoele.
Image 1. Histological view of solid galactocoele
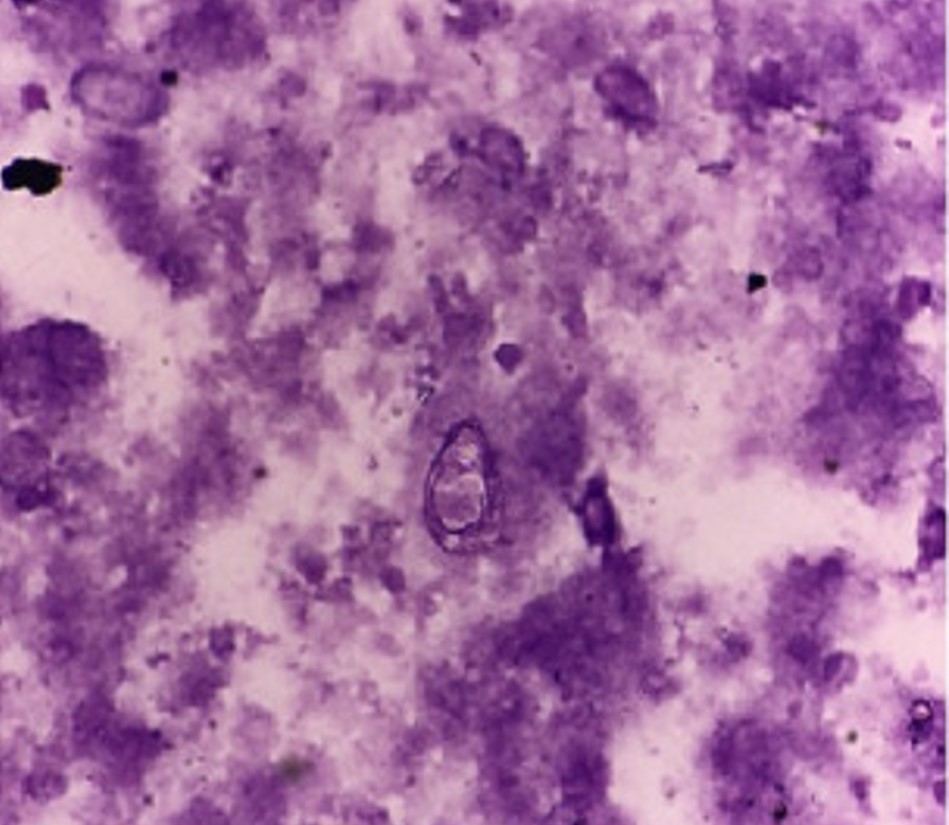
Image 2. Macroscopic view of excised solid galactocoele
References
-
Douglas PS. Re-thinking benign inflammation of the lactating breast: classification, prevention, and management. Women's Health. 2022;18:17455057221091349.
-
Stevens K, Burrell HC, Evans AJ et-al. The ultrasound appearances of galactocoeles. Br J Radiol. 1997;70 : 239-41.
-
Geddes DT. Ultrasound imaging of the lactating breast: methodology and application. International Breastfeeding Journal. 2009;4:doi:10.1186/1746-4358-1184-1184.
-
Gurumurthy RY., Shankar NS. Crystalling galactocele – histopathological diagnosis of an enigmatic entity. IJCAR 2017.
-
Varshney B, Bharti JN, Saha S, Sharma N. Crystallising galactocele of the breast: a rare cytological diagnosis. BMJ Case Rep. 2021 May 25;14(5):e242888